Selective Minimally Invasive Cryoablation as a Treatment for Premature Ejaculation
Abstract
Introduction. Premature (early) ejaculation is the second most common type of male sexual dysfunction, which has significant negative impact on the quality of life. Nowadays there is no satisfactory treatment for premature ejaculation despite its obvious need. Conservative therapy for premature ejaculation is based on the sensory decrement of the glans penis with topical anesthetics. Pharmacological effects on serotonin receptors of the central nervous system are also used with selective serotonin reuptake inhibitors. Surgical methods of treatment are based on sensory decrement of the glans penis by various methods, the main of which for the moment is selective dorsal neurotomy. The method has demonstrated good efficacy; however, it is invasive and is accompanied by the risk of complications, also the result of the intervention is not predictable. Recently, minimally invasive methods have been developed to reduce excessive sensitivity of the glans penis by temporary demyelination of the dorsal nerve of the penis using radiofrequency or cryoablation. This article presents the results of selective minimally invasive cryoablation of the penile nerves as a treatment for premature ejaculation.
Materials and methods. The retrospective study included 28 patients aged 22 to 35 years (mean age 28.7 years). All patients met CriPE (Criteria for Premature Ejaculation). The median Intravaginal Ejaculation Latency Time was 75.8 seconds (range 25 to 118 seconds). Patients completed the Premature Ejaculation Profile with a mean score of 3.6 (range 0 to 6) indicating extremely poor ejaculation control, high levels of distress, and an apparent negative impact on relationships with sexual partners. All participants underwent selective minimally invasive cryoablation of the dorsal nerves of the penis. Three months after the procedure, participants filled the Premature Ejaculation Profile again and measured their Intravaginal Ejaculation Latency Time.
Results. Average Intravaginal Ejaculation Latency Time increased from of 75.8 seconds to 227.6 seconds (+298%), the average Premature Ejaculation Profile score increased from 3.6 to 11.35 points (+315%). No significant complications were recorded.
Conclusions. Selective minimally invasive cryoablation is a promising treatment for premature ejaculation in patients who have positive response with topical anesthetics. However, additional studies with a larger number of participants are recommended.
INTRODUCTION
Premature ejaculation (PE) is known to be the second most common male sexual pathology after erectile dysfunction [1]. Conservative treatment includes oral therapy with selective serotonin reuptake inhibitors, as well as PDE-5 inhibitors [2]. In addition, local anesthetics widely used, such as 10% lidocaine aerosol, which is applied to the glans penis just before intercourse [3]. The effectiveness of sensory decrement of the glans penis with local anesthetics led to the idea of the possibility of desensitizing the glans penis with surgical techniques, such as augmentation of the glans penis with hyaluronic acid gel [4] or resection of the branches of the dorsal nerve of the penis also known as selective dorsal neurotomy (SDN) [5]. Selective dorsal neurotomy is an effective treatment for PE, but it can be accompanied by complications including the formation of neuromas [6]. Also, along the complications of SDN, excessive hypoesthesia or complete anesthesia of the glans penis, mosaic sensitivity, and erectile dysfunction should be noted. The original technique of SDN involves the complete intersection (neurotmesis) of the 50 – 70% sensory nerves of the penis. That means that restoration of sensitivity is unlikely. The results of the operation (as well as side effects) are irreversible. Some authors, such as M.M. Sokolshchik [7] and N.D. Akhvlediani [8], have improved the SDN technique by reducing the number of complications. M.M. Sokolshchik suggested do neurorrhaphy after neurotomy. Neurorrhaphy provides regeneration of sensory nerves with a gradual restoration of sensitivity, so possible side effects will be temporary. At the same time, there is a high probability of a prolonged sexual intercourse due to the phenomenon of neuroplasticity. However, the results of SDN are not always predictable, the learning curve is long, and the method is an invasive per se. The ideal method of surgical treatment of PE seems to be a less invasive easy-to-learn intervention with a low risk of complications. This method may be minimally invasive selective cryoablation of the nerves of the penis.
MATERIALS AND METHODS
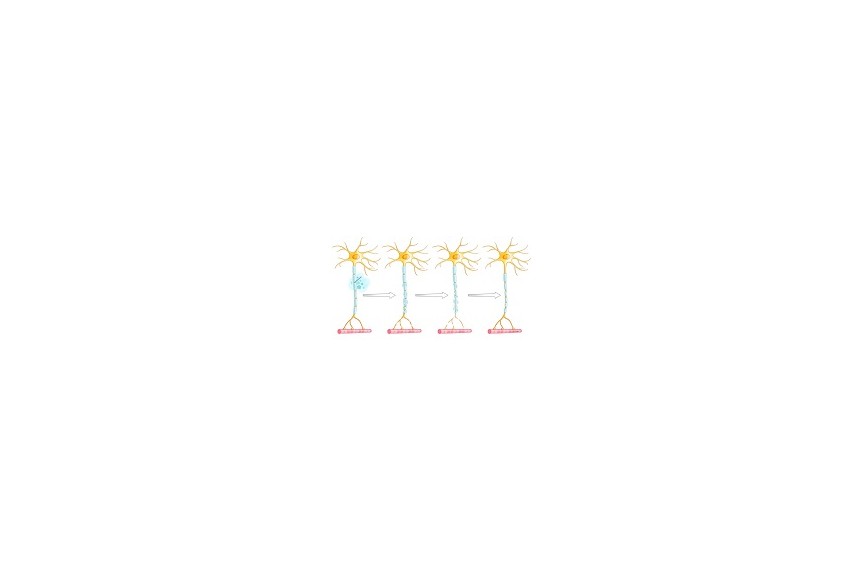
For the first time, Hippocrates reported the positive effect of cold for the reducing sensation. In recent history, the effect of low temperature on the conduction of sensory nerves was demonstrated by Cooper et al. in 1961 using liquid nitrogen (9), as well as did Amoils in 1967 using CO2 and N2O. In 1976 Lloyd et al. demonstrated that low temperature exposure on peripheral nerves caused reversible demyelination without the risk of developing a neuroma or neuritis [10]. When exposed to a temperature of -78 C, a so-called axonotmesis develops in the nerve fiber; axonotmesis is a closed intrastem nerve injury, in which its connective tissue stroma remains intact. Axonotmesis leads to a reversible impairment of nerve conduction and, as a consequence, a decrease in sensitivity in the zone of its innervation [11].
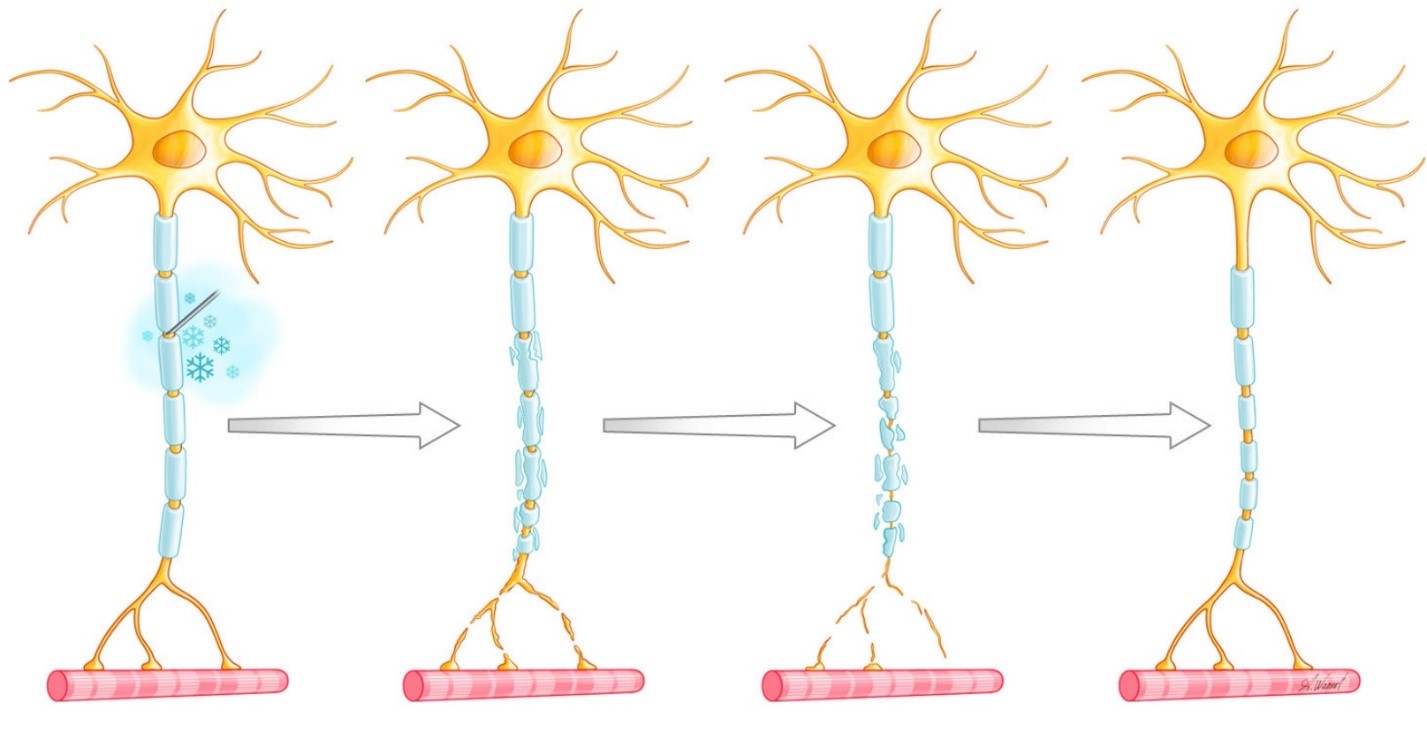
Fig. 1. Changes in the peripheral nerve after cryoablation
Subsequently, there is a slow regeneration of the nerve with the gradual restoration of sensitivity (Fig. 1). Cryoablation of peripheral nerves was widely used in the treatment of pain syndromes. Cryoanalgesia was proved to be similar in efficacy to peripheral nerve blocks with anesthetics (12).
To obtain a low temperature at the distal part of the cryoprobe, the Joule-Thompson effect is used, which is based on a decrease in temperature due to gas compression and expansion (usually CO2 or N2O). As a result, a so-called “iceball” forms on the distal part of the cryoprobe, which provides the low-temperature impact.
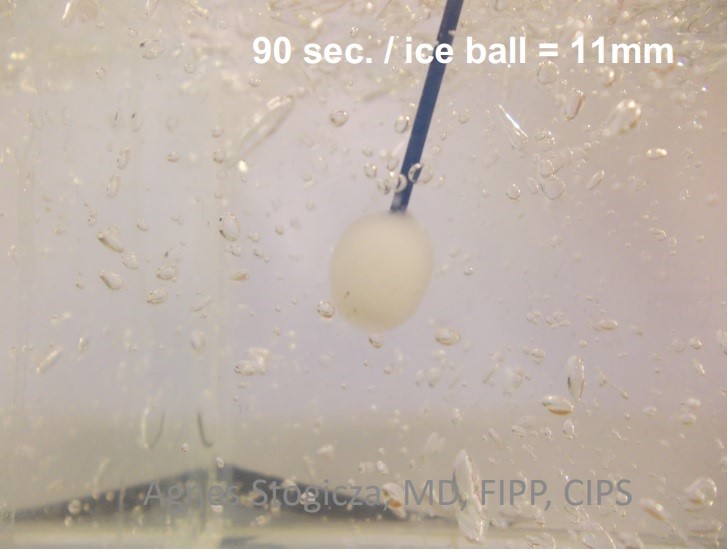
Fig.2 “Iceball” on the distal part of the cryoprobe
Photo courtesy of Agnes Stogicza
The American anesthesiologist D. Prologo published first article, dedicated cryoablation for the treatment of PE in 2013. Actively using the effect of low temperature on sensory nerves in pain syndromes, he decided to investigate the effectiveness of partial demyelination of the nerves of the penis for the treatment of premature ejaculation. CT navigation was used to localize the dorsal nerve of the penis. The branches of the pubic bone were used as landmarks. The procedure consisted of two 10-minutes freezing cycles with a 5-minutes defrosting. The results of a pilot study with 24 participants demonstrated the effectiveness and safety of the method. The mean IELT increased from 54.7 seconds to 256 seconds by day 7 post-intervention. By the 180th day, the IELT remained at the level of 182.5 seconds. Four of the 24 study participants reported temporary loss of penile rigidity. In two of them, a full-fledged erection restored on its own, two others were temporarily prescribed PDE-5 inhibitors. Three patients noted paresthesias in the glans penis; however, these symptoms resolved without further treatment [13].
Independently of D. Prologo, we have developed a SDN technique without transection of the nerves of the penis. Conduction disturbance was achieved by their cryoablation with a classic approach for SDN [14].

Fig. 3 Selective dorsal (so-called “open”) cryoablation
Photo courtesy of the authors
The original method of "open" cryoablation of the penis nerves met the requirements for reversibility of the effect, but it was an invasive procedure, like the conventional SDN. At the same time, cryoablation made it possible to perform surgical treatment of PE less invasively. So the methodology of the procedure was adjusted.

Fig.4 Selective dorsal minimally invasive “open” cryoablation
Photo courtesy of the authors
Subsequently, we continued to search other options of the technique aimed at minimal invasiveness. The main challenge in minimally invasive cryoablation of the nerves of the penis is the precise localization of the nerve. In "classic" SDN, the surgeon can see the nerve with an operating microscope, glasses or even with the naked eye. However, this requires scalping of the penis, but we suggest that less invasive procedure is preferable. It is well known that neurosurgeons and pain doctors successfully use ultrasound guidance during blockades or ablations of peripheral nerves (12). The logical decision was to use ultrasound guidance for cryoablation of the dorsal nerves of the penis. This technique was developed by the authors of the presented article and introduced into clinical practice.
Fig.5 Selective minimally invasive US-guided cryoablation of the dorsal nerve
Photo courtesy of the authors
The landmarks are dorsal arteries of the penis. Nerve usually located 3 – 7 mm laterally form artery.
The method is indeed characterized by minimal invasiveness, but it has certain inconveniences from a practical point of view, since an assistant is required for ultrasound navigation. Besides, nerves location can be variable, irrespective of artery’s site.
Another method for precise localization of peripheral nerves is electrical stimulation at a frequency of 50 - 100 Hz, which causes paresthesias in the region of innervation of the corresponding sensory nerve (15). With electrical stimulation of the dorsal nerve of the penis, paresthesias (tingling, etc.) appear in the region of the glans penis. The cryoablation device (Cryo-S Painless, Metrum Cryoflex) has a built-in electrical stimulator. After these modifications, cryoablation of the dorsal nerve of the penis is currently performed under electrical stimulation navigation and is as follows:
1. Local anesthesia of the skin with 0.5 cc 1% lidocaine solution
2. Penetration of the cannula for intravenous injection of 14G through the skin into the region of the dorsal neurovascular bundle at the 2 o'clock position – perpendicularly axis of the penis.
3. Insertion the isolated cryoprobe 18 G through the cannula.
4. Electrical stimulation with a frequency of 50 Hz to find the dorsal nerve
5. After localization of the nerve (the cryoprobe is located in the zone of maximum sensory response to stimulation), an additional anesthetic portion of 1 ml is injected through the cannula port
6. Nerve freezing: 2 freeze cycles with 2 minutes exposure and 1 minute defrost time
7. Repetition of points 4 - 6 in the position at 11 o'clock.

Fig.6 Selective minimally invasive cryoablation
Photo courtesy of the authors
It should be noted that with adequate anesthetic infiltration of the cryoablation area, the diameter of the ice ball is 15–25 mm, which means high probability of nerve involvement. In some practical cases, this gives us the opportunity to perform cryoablation of the dorsal nerve of the penis using anatomical landmarks, such as the projection of the superficial dorsal vein of the penis.
An important point of manipulation is the control of the color of the skin of the penis during the freezing cycle to avoid damage due to exposure to low temperature. It is necessary to have a warm saline solution in the operating room. Swabs with warm saline are placed on the skin of the penis when visual changes appear, such as whitening of the skin. Skin color returns to normal in a few seconds after exposure to heat. At the same time, the ice ball is preserved.
At the same time, the effect of low temperature on the cavernous bodies cannot lead to necrosis, since these tissues are abundantly vascularized. The blood acts as a heat carrier preventing the cavernous bodies and dorsal vascular bundle from excessive cooling.
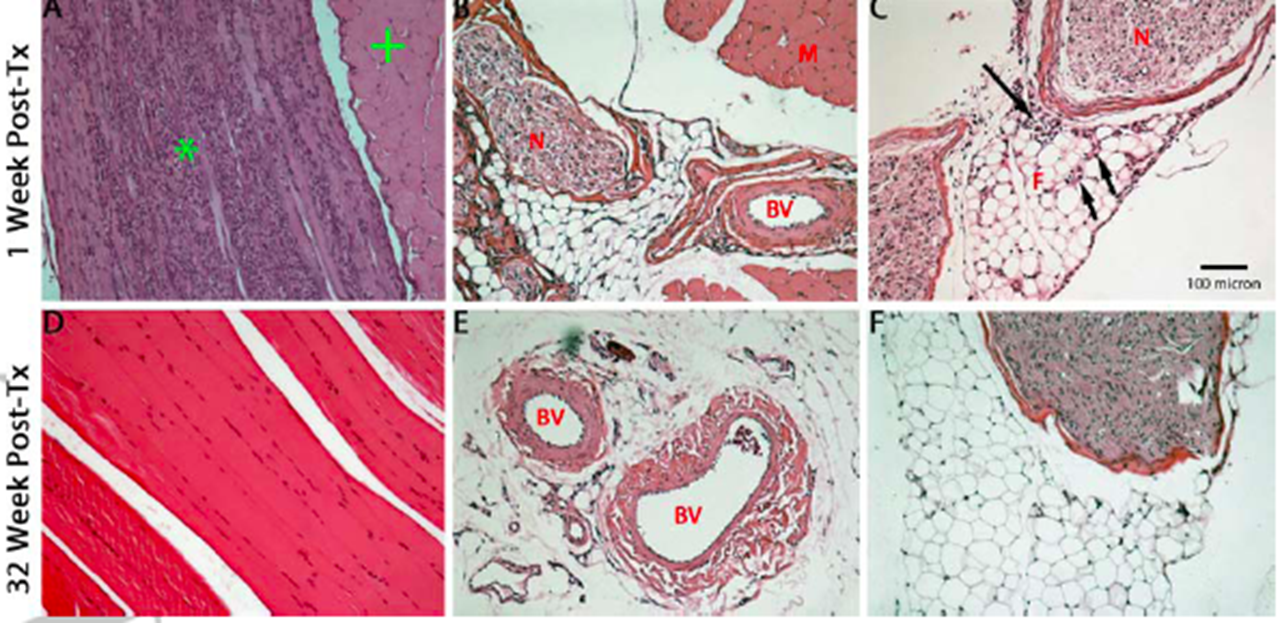
Fig.7 Hsu M, Stevenson FF. Wallerian degeneration and recovery of motor nerves after multiple focused cold therapies. Muscle Nerve. 2014. There isn’t damage of adjacent tissue
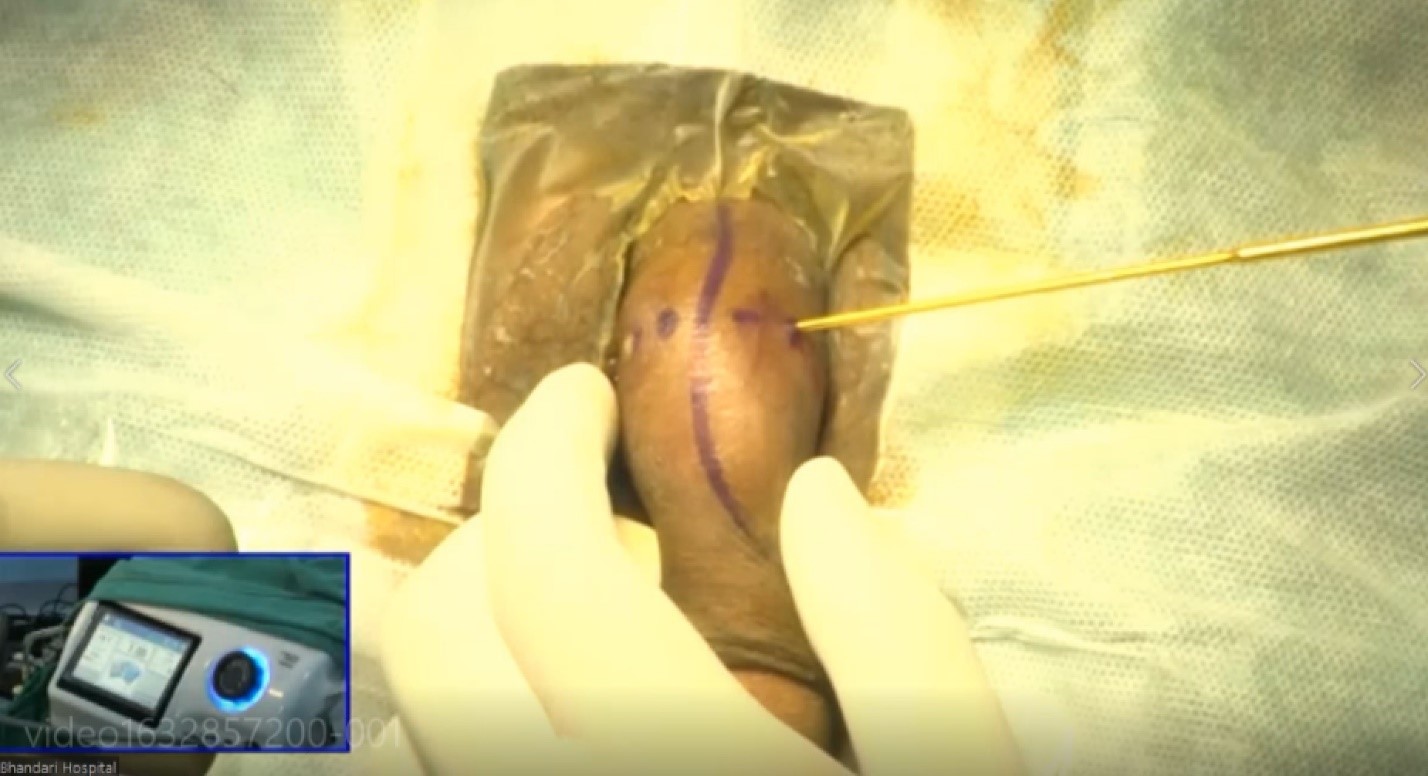
Fig. 8 Selective minimally invasive cryoablation of the dorsal penile nerve using anatomical landmarks. The “ice ball” is big enough to touch all nerves at the area from 9 till 3 clock face
Photo courtesy of the authors
RESULTS
The results of 28 selective minimally invasive cryoablations of the dorsal nerves of the penis performed at the URO-PRO Clinic (Krasnodar) and the URO-PRO Clinic (Rostov-on-Don) were analyzed. The study included the patients aged from 22 to 35 years (mean age 28.7 years).
All patients met CriPS (Criteria for Premature Ejaculation) [16]. Also, all patients measured IELT (Intravaginal Ejaculation Latency Time), which averaged 75.8 seconds (from 25 to 118 seconds); the patients also completed the Premature Ejaculation Profile – the average score before performing cryodenervation was 3.6 points (from 0 to 6 points) – which indicated extremely low control over ejaculation, a high level of distress in the study participants, and a negative impact on relationships with sexual partners [17].
|
|
|
0 |
1 |
2 |
3 |
4 |
|
1. |
In the last month, your control over ejaculation during sexual intercourse was: |
Very poor |
Poor |
Moderate |
Good |
Very good |
|
2. |
In the last month, your satisfaction with sexual intercourse was: |
Very poor |
Poor |
Moderate |
Good |
Very good |
|
3. |
In the past month, how often have you been concerned about the premature ejaculation after intercourse? |
Very often |
Often |
Moderate |
Not really often |
Never |
|
4. |
Over the past month, to what extent has the way you ejaculated quickly during intercourse affected relationship with your partner? |
Very much |
Much |
Moderate |
Not really |
Not at all
|
Table 1. Premature Ejaculation Profile
All patients underwent a test with surface anesthetics twice: a 10% lidocaine aerosol was sprayed on the glans penis before sexual intercourse for drug modeling of the operation effect. We also performed self-measurement of IELT before surgery. Patients were re-examined 3 months after the initial procedure. IELT increased from an average of 75.8 seconds to 227.6 seconds (+298%), the average Premature Ejaculation Profile score increased from 3.6 to 11.3 points (+315%).
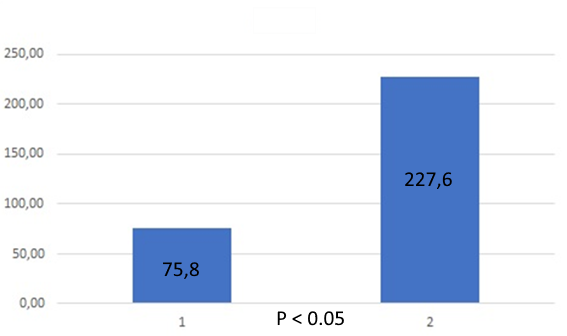
Fig. 9 IELT (sec) before (1) and after (2) cryoablation
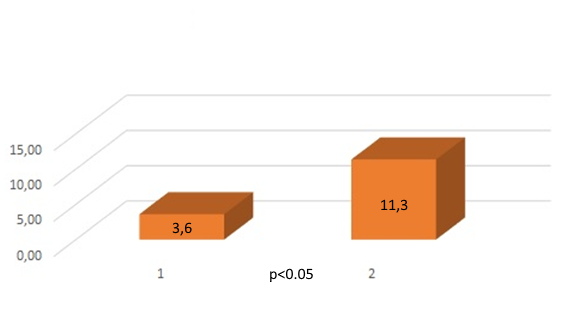
Fig. 10 Premature Ejaculation Profile (in points) before (1) and after cryoablation (2)
Evaluation was performed before surgery and 3 months after surgery. The nonparametric Mann-Whitney test was used.
For IELT calculated Uemp. = 27.5, which is less than Ucr. = 249 (p≤0.01), which means that the differences between the samples are statistically significant. For PEP, the differences between the samples are also significant: Uemp. = 0, which is less than Ucr. = 249 (p≤0.01).

Value axis:
Significant Non-significant
The obtained value Uэмп (0) is in the zone of significance.
No significant complications were registered. One patient had discomfort in the area of the glans penis within 5 days after the intervention, which was stopped by taking NSAIDs.
In general, the procedure was well tolerated by patients; all patients were discharged from the clinic on the same day. All of them tried to perform sexual intercourse during first week after procedure.
CONCLUSIONS
Selective cryoablation of the dorsal nerves of the penis is a minimally invasive and effective treatment for PE. This method eliminates the risk of neuroma formation. Since nerve demyelination is a reversible process in such cases, excessive hypoesthesia (if it occurs) is also a passing event. Selective cryoablation is much more user-friendly and can be standardized and scaled. Thus, selective minimally invasive cryoablation is a promising method for the treatment of PE.
CRYO-S ® Electric II is state-of-the-art cryosurgical device manufactured by METRUM CRYOFLEX is the next generation of apparatus used in the surgery field since 1992.

References
1. C.Carson, K.Gunn, Premature ejaculation: definition and prevalence, Int J Impot Res . 2006 Sep-Oct;18 Suppl 1:S5-13.
2. Bai Y, Pu C, Han P, Li J, Yuan H, Tang Y[7], et al. Selective serotonin reuptake inhibitors plus phosphodiesterase 5 inhibitors for premature ejaculation: a systematic review and meta-analysis. Urology. 2015 Oct;86(4):758–64.
3. Maryssa Martyn-St James et al., Topical anesthetics for premature ejaculation: a systematic review and meta-analysis, Sex Health. 2016 Apr;13(2):114-23
4. T.I. Kwak, M.H. Jin, J.J. Kim, D.G. Moon, Long-term effects of glans penis augmentation using injectable hyaluronic acid gel for premature ejaculation, Int J Impot Res. – 2008. – Vol. 20. – P. 425–428.
5. W.G. Shi, X.J. Wang, X.Q. Liang, Selective resection of the branches of the two dorsal penile nerves for primary premature ejaculation, Zhonghua Nan Ke Xu. – 2008. – Vol. 14. – P. 436–438.
6. H. J. Park Penile Traumatic Neuroma: A Late Complication of Penile Dorsal Neurotomy to Treat Premature Ejaculation// Sex Med 2016 Sep; 4(3): e221–e224.
7. Сокольщик М.М., Гагарина С.В., Вазиев Я.А. Современные методы лечения преждевременной эякуляции. Анналы пластической и эстетической хирургии. 2008;(1):84-87
8. Ахвледиани, Н.Д. Результаты 50% селективной пенильной денервации при лечении первичного преждевременного семяизвержения / Н.Д. Ахвледиани, Ю.Г. Аляев // Врач. – 2012. – No 6. – С. 37–40.
9. Cooper IS, Grissman F, Johnson R. St Barnab Hosp Med Bull 1962:11-16.
10. Cooper SM, Dawber RPR. “The history of cryosurgery.” J R Soc Med. 2001 April; 94(4): 196–201
11. Mechanism research of cryoanalgesia. Zhou L, et al S. Neurol Res 1995; 17:307-311
12. Andrea M Trescot et al. Ultrasound-guided percutaneous cryoneurolysis providing postoperative analgesia lasting many weeks following a single administration: a replacement for continuous peripheral nerve blocks: a case report. Korean J Anesthesiol., 2017 Oct., 567-570
13. J. David Prologo et al. Percutaneous CT-guided Cryoablation of the Dorsal Penile Nerve for Treatment of Symptomatic Premature Ejaculation//J Vasc Interv Radiol 2013; 24:214–219
14. Миркин Я.Б., Невский А.А. Современные методы малоинвазивного лечения преждевременной (ранней) эякуляции. Экспериментальная и клиническая урология 2022;15(2)110-118; https://doi.org/10.29188/2222-8543-2022-15-2-110-118
15. Montgomery SJ, Raj PP, Nettles D, Jenkins MT: The use of the nerve stimulator with standard unsheathed needles in nerve block. Anesth Analg 1973;52:827–831.
16. Ибишев Х.С., Гусев А.А., Чибичян М.Б. Преждевременная эякуляция. Учебно-методическое пособие. Ростов-на Дону, 2016. 84 с.
17. Donald L. Patrick et al. The Premature Ejaculation Profile: validation of self-reported outcome measures for research and practice, BJU Int. 2009 Feb;103(3):358-64.