CRYOABLATION OF PENILE NERVES FOR PREMATURE EJACULATION TREATMENT: HOW IT WORKS AND WHY IT’S SAFE.
Currently, most surgical treatments for premature ejaculation are targeted at reducing the sensitivity of the penis.
The most common of these is selective dorsal neurotomy (SDN) – transection of penile nerves.
The method is effective, but non-reversible. It means, that SDN could leads to total lifelong anesthesia of the penis with risk of erectile dysfunction.
In the picture below shows the degree of nerve damage by Seddon:
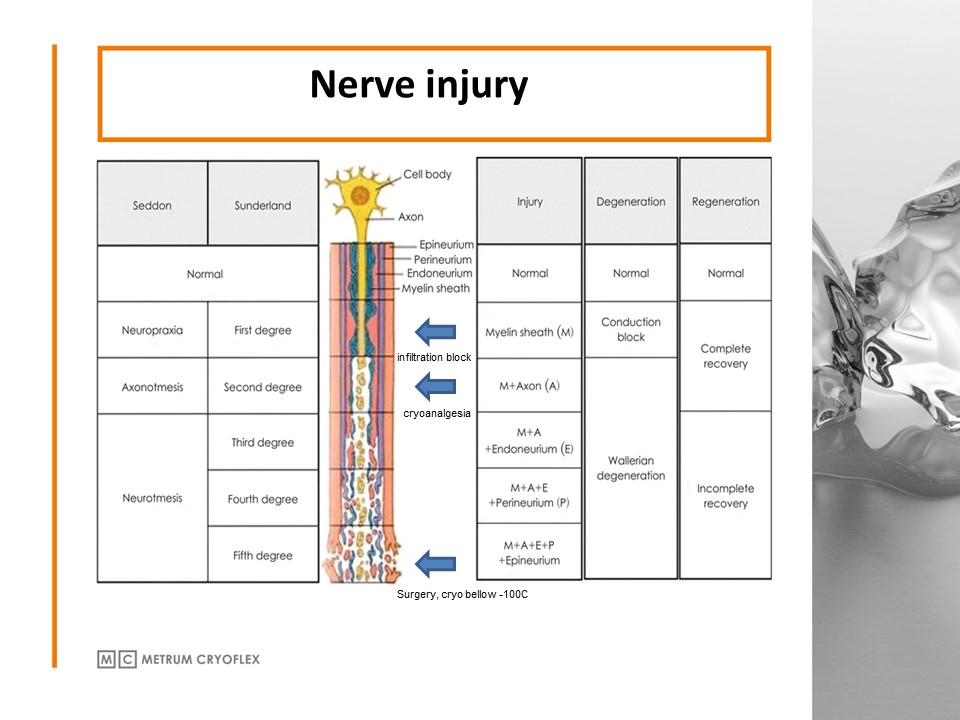
Nerves transection (SDN) is 3rd – 5th degree – neurotmesis. The nerve is completely destroyed, regeneration is impossible.
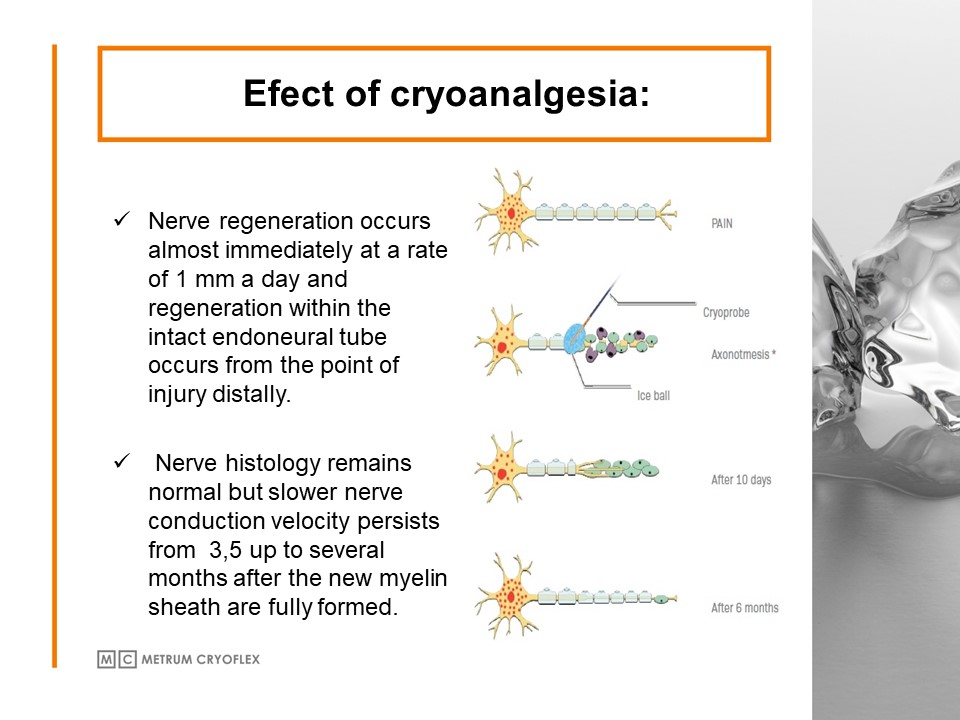
Cryoablation leads to 2nd degree – axonotmesis. There’re injury of myelin and axon, but other nerve’s structures stay intact.
It means, that axonotmesis is temporary injury of the nerve. Regeneration is not only possible, it is inevitable.
Hence, cryoablation looks safer in comparison with nerve transection.
But what about safety of cryoablation per se? Does the surrounded tissue (arteries, veins, cavernous bodies) stay intact?
In the picture below shows physics of cryoablation.
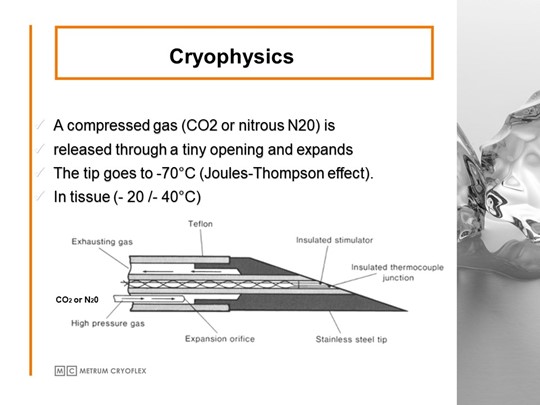
There is low temperature on the cryoprobe tip leads to ice ball formation.
The size of ice ball depends of freezing time.
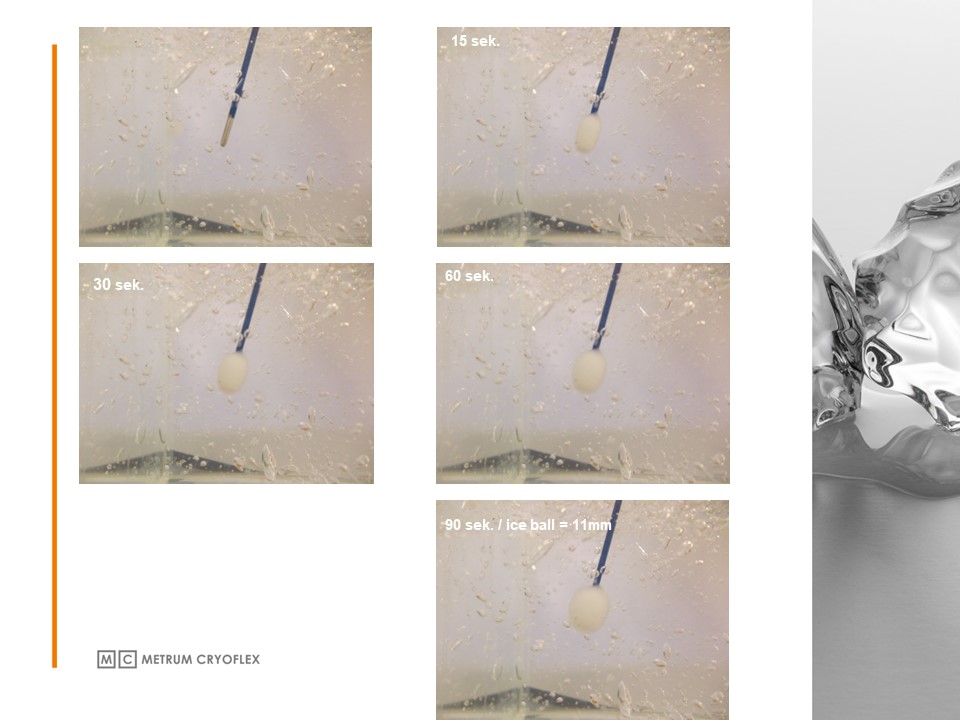
The rather large size of the ice ball means that the cryoprobe may not touch the nerve directly.
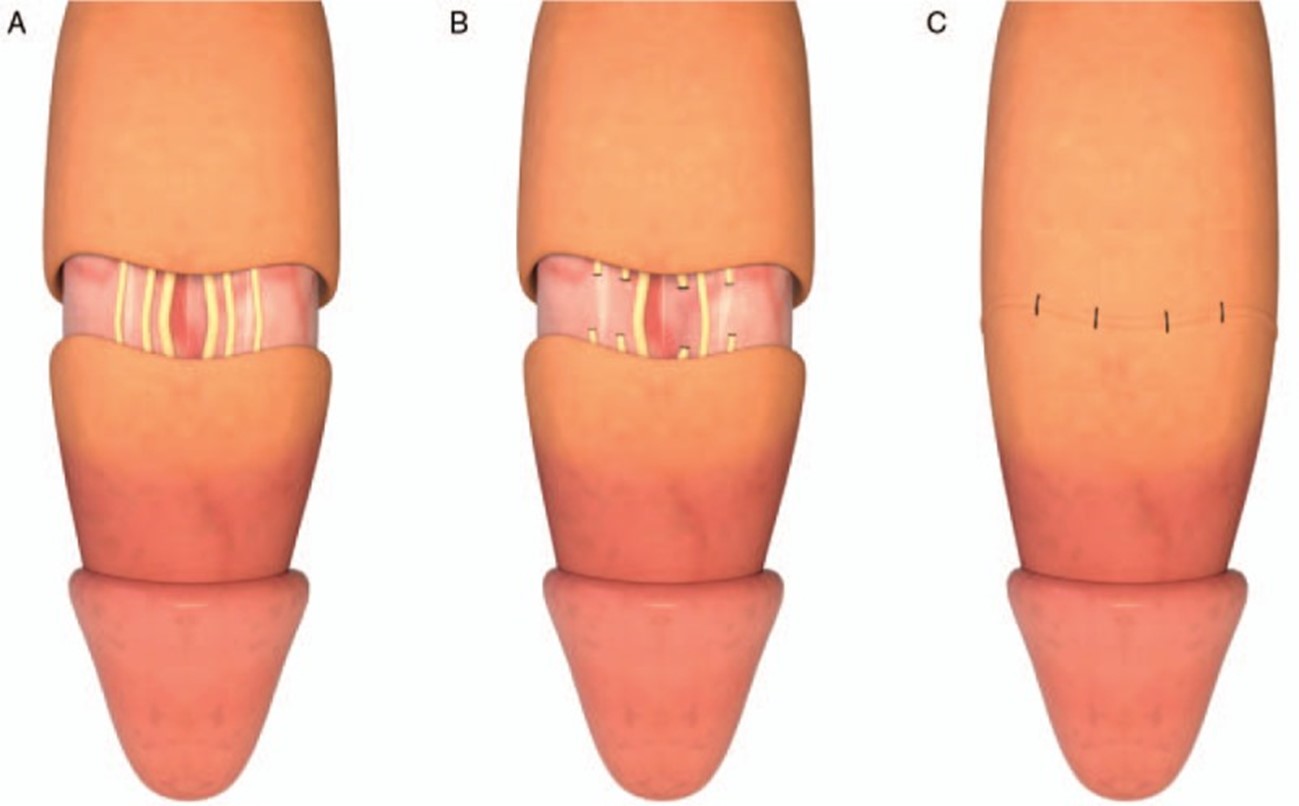
In the figure below, you can see the results of histological examination of the surrounding tissues after nerve cryoablation.
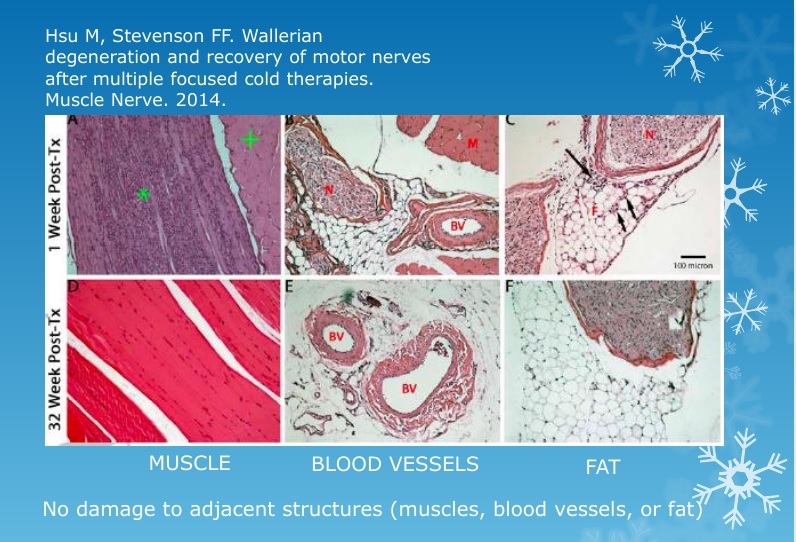
There is not damage of adjacent structures.
Thereby, cryoablation is an absolutely safe method of reducing the sensitivity of the penis.
CRYO-S ® Electric II is state-of-the-art cryosurgical device manufactured by METRUM CRYOFLEX is the next generation of apparatus used in the surgery field since 1992.

